Surgical Procedures
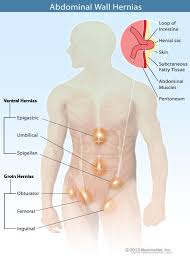
Hernia
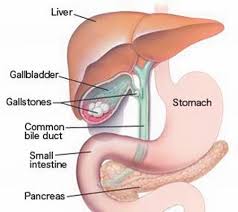
Cholecystectomy (Gallbladder)
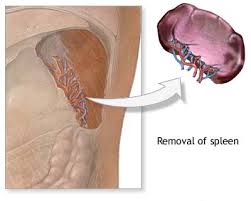
Splenectomy
Gastric Tumors

Reflux
Diaphragmatic hernias and reflux disease
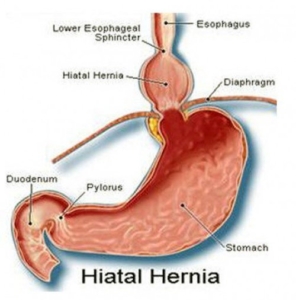
What: The stomach is characterized by an acidic environment. The lower esophageal sphincter functions as a physiological barrier between the acidic stomach and the neutral esophagus. In situations where the sphincter’s function is compromised, or when there is a diaphragmatic hernia, acidic fluid washes the esophageal mucosa (reflux) causing esophagitis and eventually may cause metaplasia.

Symptoms: Patients suffering from reflux will often complain of heartburn, regurgitation, chest pain and sometimes difficulty swallowing.
Diagnosis: Diagnosis of reflux disease (GERD) is based several studies including gastroscopy, barium swallow, esophageal manometry and ph-metry of the esophagus.
Surgery: Some of the patients suffering from GERD will be referred for surgery. The goal of surgery is to ‘tighten’ the sphincter and repair the diaphragmatic hernia. The procedure is performed under general anesthesia using the laparoscopic approach. A laparoscopic Nissen fundoplication is usually performed.
Hospital Stay & Recovery: Length of stay following laparoscopic diaphragmatic hernia repair ranges from 3 to 5 days, and depends on the complexity of the hernia and the patient’s overall condition.
Make An Appointment
Get hafnia and hithayvut from your family physician.
Gather laboratory results, imaging studies such as ultrasound and CAT scan.
For public appointment call 02-5842111
For private appointment call 02-6778899